In the last 40 years, there has been big progress with regards to internal fixation of the hand and wrist. Studies have shown that in order to achieve early regaining of pre injury mobility and good functional outcomes, a stable fixation with good soft tissue handling is primary. Locking system of Screws and plates used in the hand were first established for long bone fixations. Where it acts as an internal – external fixator. Also known as a fixed-angle construct. This type of fixation has developed a growing popularity in the fixations of periarticular, periprosthetic and complicated multifragmentary meta and diaphyseal fractures. Their indications have now included hands and wrist as well.
There has been a rise in the number of companies providing implants that are specifically designed as fixed angle constructs a result of increase in the interest of hand as an emerging specialty. The different varieties of these fixation devices reflects the preference of orthopedic surgeon performing complex cases with a range of indications including periarticular fixations ,corrective osteotomies and revision surgeries for a post operative deformed hand . As per indication these locking plates can be used to provide either a rigid or stable fixation.
The use of Locking plates in the hand is a relatively new concept when compared to its uses in the fixation of long bones like upper end humerus, tibia or distal end femur. In due course of time and experience, the fixed angle locking plates are destined to replace the more cumbersome fixed angle blade plates.
The discussions regarding indications and contraindications of the locking plate innovations have been limited to the lower end of ulna and bones of the hand.
Biomechanical distinctions
Non locking compression plates
Standard non locking plates are dependent on the friction forces in the bone-plate interface. This is to resist deformation due to rotational, torsion and bending forces across the new construct over the reduced fracture. This mainly depends on the screw torque generated. Conditions where fracture affects osteoporotic bones, multiple fragmentations, bone loss and pathological bones reduce the screw thread purchase and stability is compromised. There is also need for extensive soft tissue and periosteal stripping for increasing the bone to plate contact which in turn is detrimental for fracture healing.
Locking plate constructs
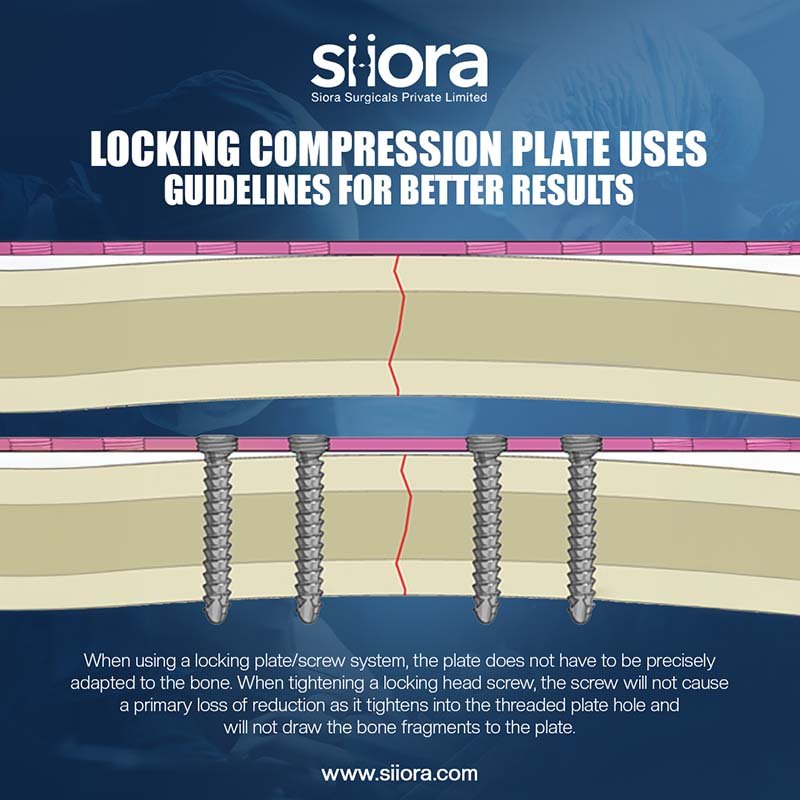
Previously in the above given conditions attempts were made to improve the fixation by using bone cement and special screws and plates. However, it has been recently reviewed and improved by AO/ASIF group. In the Synthes fracture fixation system, the locking screw heads are conical with threads that lock into corresponding screw hole threads that are recessed within the body of the plate. In general, fixed angle locking constructs prevent screw toggling within the plate and act as a single unit. They preserve the periosteal vascularity and act similar to an external fixator in an internal environment.
The locked screws in an angular stable manner dissipate the forces evenly along the individual screws and prevent concentration of loads at one screw. They act in parallel as compared to serially in non locking constructs. If they do fail, it is as a whole unit rather than individual unlocked screw toggling in the screw hole.
In areas of multiple fragments or bone is lost, a locking plate may be used to bridge across the concerned fractured area and thus avoiding compression. This is advantageous as it doesn’t disturb the vascularity of the bone fragments while giving a relatively stable fixation. Healing occurs by callus formation due to micro motion allowed across the fixation. Another advantage is an option to use non locking screws in compression mode where necessary. This is due to combination holes are provided in it.
Combi-hole plates are the latest in locking plate innovation giving the orthopedician, the option to use either screws, where deemed fit. More specifically it has a dual purpose of anatomic reduction and fixation in compression mode or a stable fixation in a bridging mode.
When to use it
Some of the uses of these plates in relation to the hand include badly comminuted fractures of distal ulna or radius, juxta-articular metacarpal or phalanx fractures, osteoporotic bones, ununited fracture fixation, arthrodesis and deformity correction in hand.
When not to use
If there is simple diaphyseal or simple articular fracture in a bone with good bone density and when cost is a factor in management of the patient, a non locking plate will very much suffice.
Hand consists of closely packed nerves and vessels in between a tight space shared by multiple tendons. Here the advantage of percutaneous extraperiosteal plating cannot be made use of and has to be avoided.
Specific indications by regions of hand
Lower end ulna:
5-7 percent of patients with unstable lower end radius fracture are associated with unstable lower end ulna fracture. This type of fracture requires good reduction and stable fixation especially the DRUJ. Regaining the ulnar height to pre operative levels is a priority to prevent non-union, distal radio-ulnar joint instability and early degenerative changes.
Good to excellent results have been achieved with mini-fragment (2mm/2.4mm/2.7mm) Y, T or L shaped locking plates in similar scenarios as mentioned above. Surgical plane is developed between the FCU and the ECU carefully, avoiding damage to the dorsal ulnar sensory nerve. Damage to the TFCC has to be avoided using intra-op imaging whenever necessary. The shape of the plates allow the ends to be bent to wrap around the ulnar head adding stability, while allowing the screws to be locked in different angles.
Another advantage in the ulna head is the use of locking bolts in uni-cortical fashion in order to avoid entry into the sigmoid notch. This is crucial to avoid any hindrance to forearm rotation.
Few significant problems do exist with these plates and it includes loss of fixation in difficult fractures, palpable implant/screws, malreduction which may require a re-do surgery.
Fractures of the metacarpal and phalanges
Extra-articular fractures are associated with multiple fragmentations, loss of bone, comminuted cortex and surround soft tissue damage. Invariably they will require a rigid fixation with accurate reduction in restoring height, angular and rotational alignment along with soft tissue reconstruction as it is prime importance to regain pre operative mobility as soon as possible.
Locking plates are useful in this region for its ability to provide stable fixation. This too without disturbing the periosteum and also ability to bridge across comminution. Approach to the metacarpals is via a tendon splitting or retracting the extensor tendon. A mid-lateral plate position is preferred.
Peri articular fracture of hand bones
Fractures around the condyles are not stable due to the pull of collateral ligaments, creating a rotational and angular deformity. Usually they are associated with metaphyseal comminution. A kirschner wire or screw fixation may not do justice. Approach for ORIF requires going in between the central slip and lateral band/ reflection of the central slip. 1.5mm mini condylar blade or locking plate applied dorsally or laterally is ideal in such scenarios. It is for providing stable support for post-op rehabilitation. Damage to the vascular structures i.e. collateral ligaments and impingement can be avoided by positioning the plate laterally.
Base of phalanx fractures may have articular involvement with impaction. Approach may be taken either tendon splitting or tendon retracting. Impaction is elevated and fracture secured with a k-wire temporarily. Definitive fixation is done with dorsally applied t or y shaped plates and angular stable screws providing support to the comminuted metaphysis. Single screw in the peri-articular region with eccentric screw in the cortical bone may result in faulty alignment and rotation.
Specific fracture like Rolando, Bennets and 5th MC require careful planning for plate position. Dorsally applied plates resist deformity in volar comminution due to their angular stability.
Reconstructions in hand
Indications for surgery include non unions and angular/ rotational deformity mal-unions having functional limitations. Challenges faced by hand surgeons are the presence of old scar and soft tissue adhesions adding stress on the corrective fixations. Locking plates provide angular stability which allow for early rehabilitation in such scenarios.
Non unions and delayed unions are rare in the hand. However if they cause functional limitations, studies have shown better outcomes with surgery using locking plates and screws fixations. For example: straight or H shaped plates for tubular bones and mini-condylar plates for peri-articular and metadiaphyseal regions. Addition of corticocancellous grafts at the site of non unions can be secured with locking screws.
Some studies have shown good to excellent outcomes in 95-97% of corrective osteotomies for phalanx mal-unions in isolation, but it went down to 63-65% when soft tissues were reconstructed. Hence a rigid angular stable fixation helps in early movements and improves recovery.
Indications for arthrodesis include an immobile and painful joint next to juxta articular non-union. Locking plate constructs allows both fusion of the joint as-well-as correction of the non-union with debridement and bone grafting.
Complications
There are similarities in the type of complications between locking construct and regular non locking plating in the hand. However the few complications specially seen in locking construct are as follows. When the screw threads and the plate threads are not matching while inserting it. It can lead to disengagement and failure post operatively. Screws can break from the plate post operatively during loading, if the rotational force while application of screw is not adequate. If the correct length of plate is not used for the fracture concerned. The working length become inadequate and the mechanism is bound to fail. These are surgeon dependant causes. Extremely poor bone quality and badly fragmented fracture is some of the patient related causes of complications
When contouring a plate, care must be taken to make sure it is a perfect fit. The locking sleeves must also be secured into the plate before contouring to prevent loss of locking mechanism. Non locking compression screws must be inserted to achieve compression prior to placing locking screws. If these three technicalities are not followed correctly it can lead to non-union, mal-union or implant breakage.
Siora Surgicals
Siora Surgicals has developed the mini-fragment hand locking compression plate (LCP) fixation systems in titanium only. Self-tapping cortical and locking screws are available in the 2.7-mm, 2.4-mm, and 2.0-mm mini-fragment hand trays. The LCP plates have combi-holes that can accommodate either cortical or locking screw fixation through the same hole. Here, the locking screw heads are conical with threads that lock into the screw hole threads. These plates have monoaxial locking screw angles. It defines the trajectory of the locking sleeve insert into the locking side of the combi-hole. The 1.8-mm locking subarticular buttress pin will be required with the 2.4-mm condylar plate. These Plates are available in straight, Y-, T-, and H-shapes. Plate cutting and additional contouring are possible with notched plates. These plates are low-profile (plate thickness range, 0.7–1.25 mm) and hence, it makes periosteal closure around the implant easier.
Conclusion
The angular stable locking constructs in the hand is a versatile technology which allows for fracture fixations, deformity corrections, joint fusions in variety of scenarios where there is bone loss, opposite side cortical discontinuity and juxta articular comminution. Its applications have only recently become popular and long term studies are anticipated in the near future. However what we do know is, proper understanding of principles of fracture fixation and accurately following the biomechanics of the locking plate constructs, go hand in hand to provide a successful outcome.