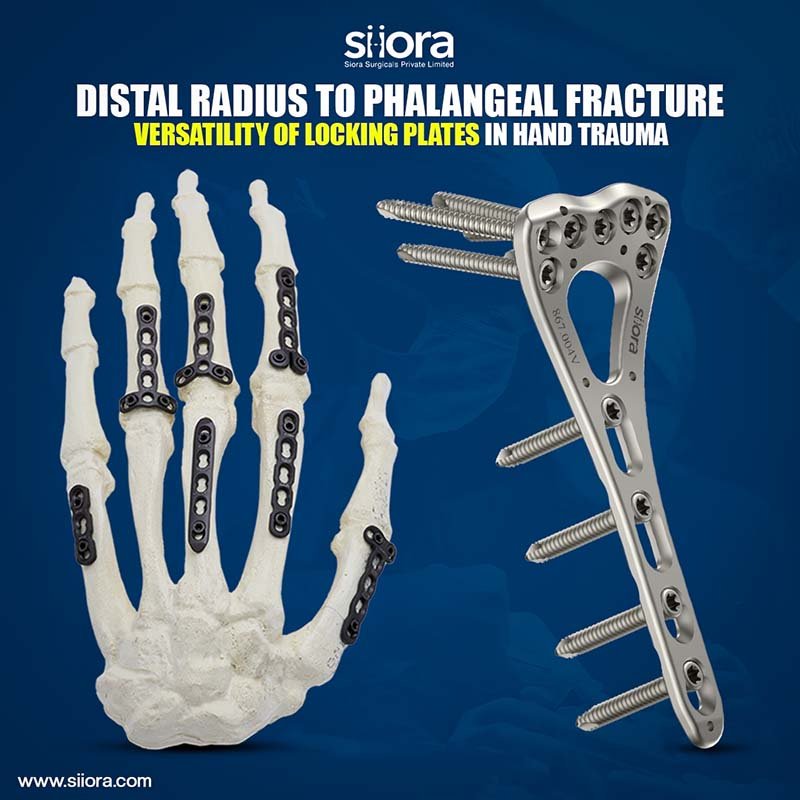
The human skeleton made of 206 individual bones that perform various important functions, protection, movement, including support, storage of minerals, and formation of blood cells. To ensure that the skeleton retains its ability to perform these functions, and to reduce disfigurement and pain, bones that become fractured should be repaired promptly and properly. Typically, a fractured bone is treated using a fixation device or an orthopedic implant, which reinforces the fractured bone and keeps it aligned during the healing process that can be accessed from Orthopedic Products Manufacturers. Fixation devices and orthopedic implants may take a variety of forms, including casts and fixators for external fixation, and bone plates, and rods, and/or fasteners (screws, wires, pins, etc.) for internal fixation, among others.
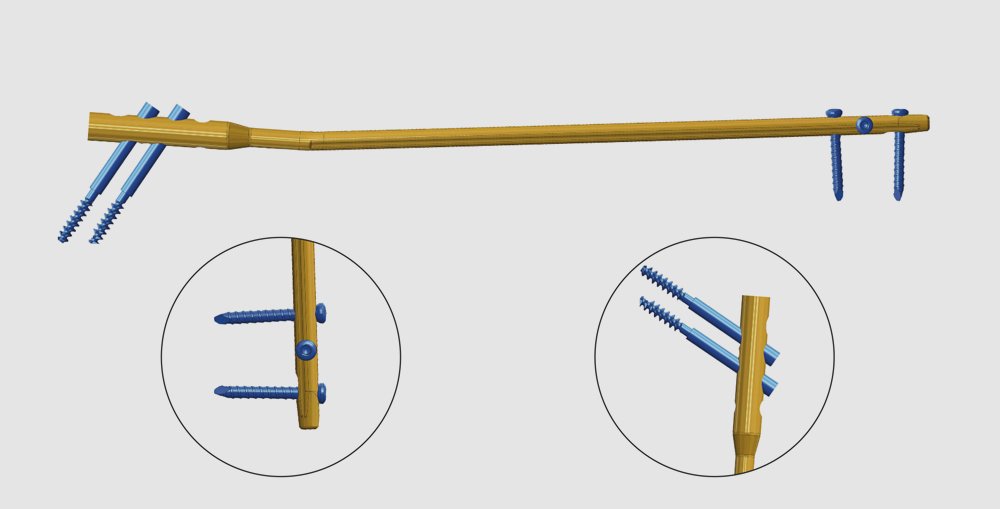
Orthopedic rods may function as fracture fixation devices (e.g., intramedullary nails) and/or prosthetic devices (e.g., stem portions thereof), among others, received in the medullary canal of a broken and/or cut bone. For installation of the accessed from an end and/or side of the bone with an instrument such as an awl, saw, or drill. The medullary canal also may be prepared to receive the orthopedic rod, for example, by reaming and/or broaching to enlarge and/or shape the canal. After placement of a rod into the canal, the rod may be secured in position using fasteners, for example, by attaching the rod to only one fragment or, in the case of fixation, to two or more bone fragments disposed on opposing sides of a break or cut in the bone. the rod, therefore, may include a plurality of apertures (holes) that receive threaded fasteners, such as bone screws, which may be anchored in the bone adjacent to each aperture via an external thread.
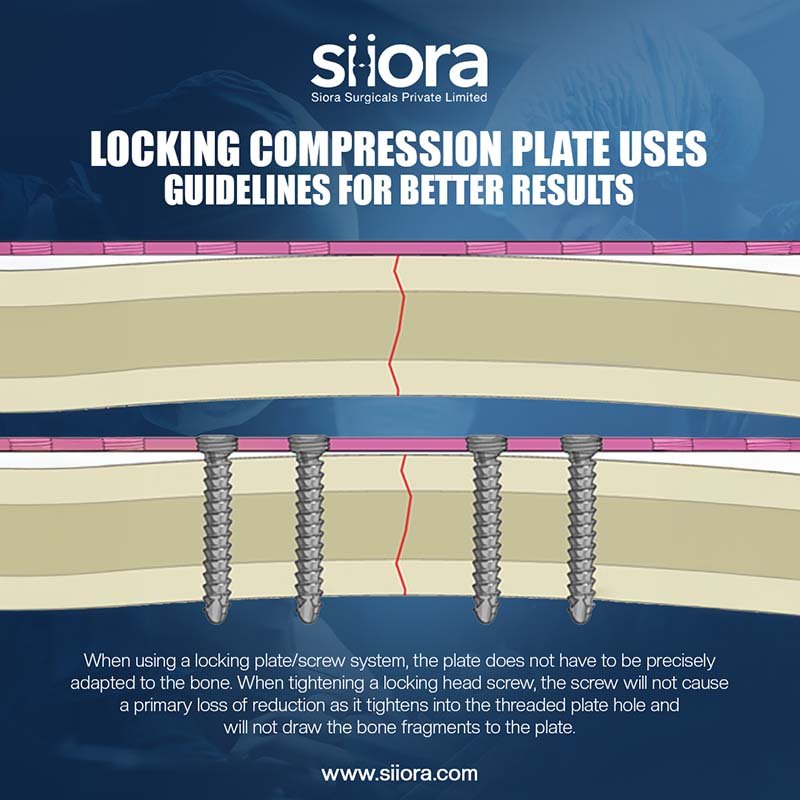
Each aperture within a rod may be locking (e.g., with a thread) or nonlocking (e.g., without a thread). A locking aperture may engage a suitable corresponding fastener such that the fastener’s translational movement in both opposing directions along the aperture is restricted; in contrast, a nonlocking aperture usually permits this translational movement. Of these two types, nonlocking apertures may be relatively easy for an orthopedic surgeon to use because a nonlocking aperture usually can receive a threaded fastener that is aligned with the aperture, irrespective of the relative rotational disposition of the aperture and the fastener. However, nonlocking apertures may be less effective for fixing the threaded fasteners, rod, and/or bone in position.
Locking apertures of a rod may be more difficult for a surgeon to use. Because a locking aperture is spaced from the bone surface by bone, a threaded fastener that is advanced rotationally into the bone from the bone surface may arrive at the locking aperture at an unsuitable rotational (and therefore axial) disposition relative to an internal thread of the aperture. Therefore, the threaded may be hard to turn and/or may create an undesirable sound (such as squeaking), among others, during fastener advancement after the fastener is forced into registration with the locking aperture. Moreover, a bone may be damaged (e.g., a thread femoral formed in the bone may be stripped) as the threaded fastener is forced into registration. This problem may be compounded by bone screws having a deep external thread (and therefore a relatively large pitch) for engagement with the cancellous bone.