




In orthopedic surgery, precision, stability, and minimal invasiveness are key to successful fracture fixation and patient recovery. Among the most widely used implants for internal fixation are cannulated screws and Herbert screws, each designed for specific anatomical and clinical requirements. Though they may appear similar at a glance, their structures, mechanisms, and uses vary significantly. Understanding these differences is crucial for surgeons when selecting the right implant for optimal outcomes. This blog provides a comprehensive breakdown of cannulated and Herbert screws, including their types, design features, clinical uses, and how they function in bone repair, to help clarify their roles in modern orthopedic procedures and ensure informed decisions in surgical practice.
What is the Difference Between Cannulated Screws and Herbert Screw?
Cannulated screws and Herbert screws are both orthopedic implants used for internal fixation of fractures. While they share some design elements, such as the option for cannulation (a hollow core to accommodate a guide wire), they serve different purposes and have distinct structural differences.
- Cannulated screws are primarily designed for guided insertion using a guide wire, offering ease of placement, particularly in complex fracture regions.
- Herbert screws, on the other hand, are headless compression screws designed to create interfragmentary compression. These are especially useful in articular fractures where prominence of the screw head must be avoided.
Now, let’s explore both in more detail.
What are Cannulated Screws?
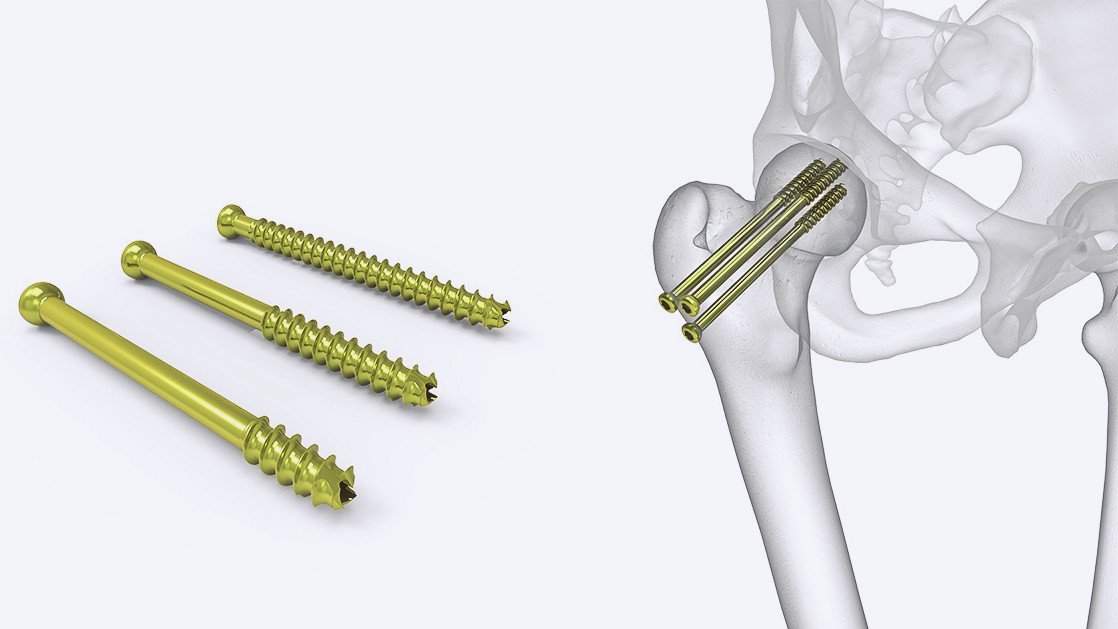
Cannulated screws are orthopedic screws designed with a central hollow channel to be inserted over a guide wire. This allows for highly precise placement, especially in metaphyseal and epiphyseal bone areas. By enabling controlled alignment and fixation, they significantly reduce the risk of misplacement compared to solid screws.
A guide wire:
- Provides a clear visual path for screw insertion.
- Helps maintain fracture reduction during the procedure.
- Can be repositioned without enlarging the bone hole or weakening bone integrity.
Cannulated screws are typically used with additional cannulated instruments including drills, taps, and screwdrivers. The screws are available in various sizes and head types to accommodate different anatomical requirements.
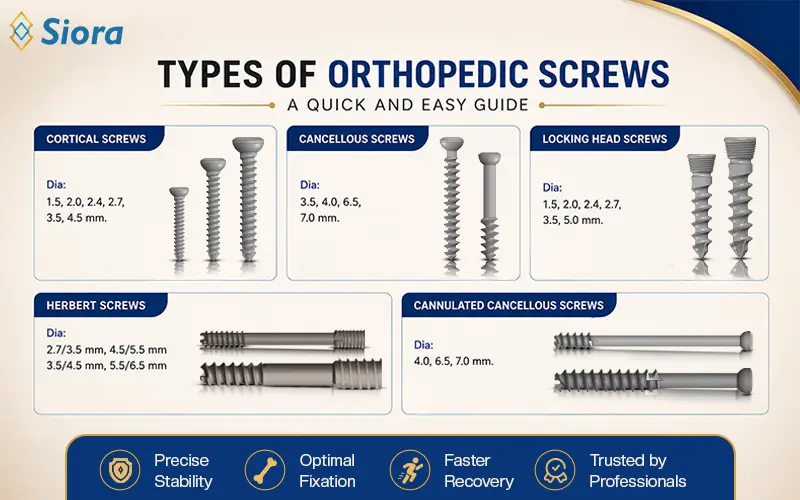
Types of Cannulated Screws
Cannulated screws come in two main types based on their size and application:
Large Cannulated Cancellous Screws
Used for femoral neck, tibial plateau, and femoral condyle fractures.
Small Cannulated Cancellous Screws
Applied in fractures of the distal radius, distal humerus, carpal scaphoid, and both distal and proximal tibia.
Additionally, based on their head design:
- Internal hex head screws have a recess for a slim, cannulated screwdriver.
- External hex or square head screws offer better coupling strength but may be harder to remove if bone grows around the head.
Cannulated Screw Uses
Cannulated screws are widely used in:
- Percutaneous fracture fixation
- Metaphyseal and epiphyseal bone fracture repair
- Fixation of non-displaced fractures
- Minimally invasive surgeries
Their precision and minimally invasive nature make them ideal for procedures requiring guided fixation, especially where preserving bone strength is crucial.
Key benefits include:
- Easier repositioning using guide wire
- Less bone damage during screw placement
- Improved fixation control with reduced surgical trauma
What is a Herbert Screw?
The Herbert screw is a headless compression screw designed specifically to provide interfragmentary compression across bone fragments. It achieves this through differential thread pitches at each end, the leading threads (near the tip) have a coarser pitch than the trailing threads.
This design ensures:
- As the screw is tightened, the two bone fragments are drawn together.
- Compression is generated internally without the need for a screw head.
- The screw can be fully buried beneath cartilage or bone without protrusion.
The Herbert screw is especially useful in intra-articular fractures, such as those in the carpal scaphoid or radial head, where any protruding hardware can impede joint function.
Types of Herbert Screws
There are two main variations of Herbert screws:
Standard Herbert Screw
Solid design used for open surgical fixation, where guide wire placement is not necessary.
Cannulated Herbert Screw
Hollow-core design allows placement over a guide wire.
Enables percutaneous procedures with better alignment and reduced bone damage.
The cannulated version is particularly advantageous for minimally invasive fracture treatments, as it preserves the structural integrity of cancellous bone.
Herbert Screw Uses
The Herbert screw is particularly effective in areas where traditional headed screws might interfere with joint movement or become prominent. Common indications include:
- Carpal scaphoid fractures
- Radial head fractures
- Capitellar fractures
- Osteochondral fractures
- Osteochondritis dissecans
- Small joint arthrodesis
Key advantages:
- Promotes interfragmentary compression
- Avoids need for screw head protrusion
- Allows insertion through articular surfaces
- Reduces soft tissue irritation
Additionally, the cannulated Herbert screw enables percutaneous insertion, minimizing surgical exposure and soft tissue trauma, while speeding up recovery time.
Conclusion
Both cannulated and Herbert screws play a crucial role in modern orthopedic surgery, especially for precise and minimally invasive fixation.
- Cannulated screws offer guided placement over a wire and are ideal for percutaneous fixation of metaphyseal and epiphyseal fractures.
- Herbert screws, particularly the cannulated version, provide compression without a protruding head, making them perfect for delicate joint areas and intra-articular fracture fixation.
Understanding their differences and applications allows orthopedic surgeons to choose the most effective implant for optimal healing and biomechanical stability.